To Inject or not to Inject
Case Study:
Dr Robyn Troutbeck
Presentation
The following patient was referred by the GP with a recent loss of vision in the LE. He is a poorly controlled diabetic.
This is his RE. Vision is 6/6.

This is his LE. Vision is 6/60.
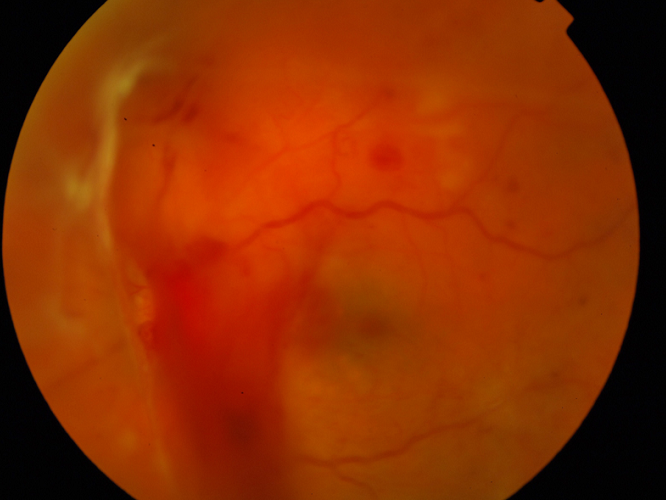
What can you see?
Click for answer.
He clearly has proliferative disease with NVD and vitreous haemorrhage with some fibrosis and possible tractional detachment nasal to the disc.
What investigation would you perform?
Click for answer.
Take a fluorescein angiogram.
The RE is presented below.
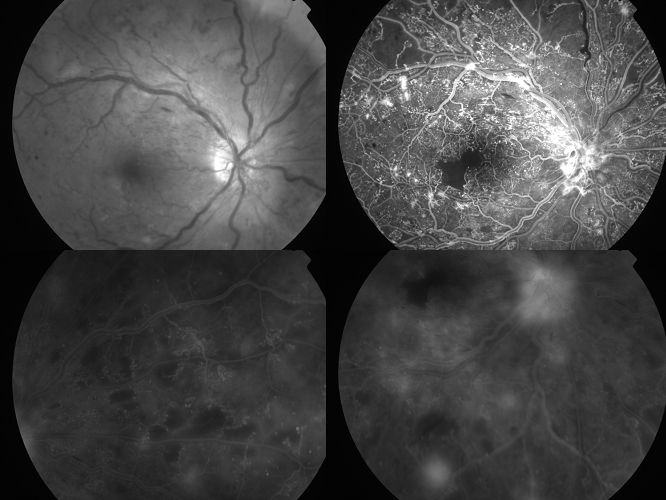
What do you see?
Click for answer.
He has NVE/NVE and macula ischaemia.
What to do next?
Click for answer.
He needs urgent treatment. Given, he has no macula oedema, standard of care currently is to start PRP in both eyes. He needs to optimize his blood sugar, blood pressure and cholesterol.
The DRCR.net Protocol S has published 2year results looking at the use of ranibizumab vs PRP for proliferative diabetic retinopathy. The results are promising and the FDA has now approved lucentis in the US for this use. In Australia, we can use off label Avastin only to treat proliferative disease. One of the biggest problems with anti-VEGF treatment is the need for regular injections and therefore close follow-up. Typically, this is a difficult group to managed due to multiple medical problems related to poorly controlled diabetes. The benefit of the laser, is that we can complete the PRP in 3-4 sessions and prevent severe vision loss. However, this is at the expense of peripheral vision and night vision loss. We eagerly await the DRCR.net 5 year results.